
Intermediate Care / Community Reablement
Intermediate care is an NHS and Social Care programme of active rehabilitation.
Intermediate care supports people to remain at home in crisis, or return home after hospital stay. Where possible, the service will provide this support in the person’s own home. If the person can’t be supported at home, then their recovery will be supported in an intermediate care bedded, reablement facility.
Decisions about a person’s long term care needs are made outside of an acute hospital setting. The maximum length of stay in intermediate care settings is expected to be up to 6 weeks but may be shorter depending upon how people recover. This period of up to 6 weeks is referred to as the ‘reablement period’.
People should be supported to be discharged to the right place, at the right time and with the right support that maximises their independence and leads to the best possible sustainable solutions.
Under the ‘discharge to assess’, ‘home first’ approach to hospital discharge, the majority of people are expected to go home [to their usual place of residence] following discharge. This model is built on evidence that the most effective way to support people is to ensure they are discharged safely when they are clinically ready, with timely and appropriate recovery support if needed. An assessment of longer-term or end of life care needs should take place once they have reached a point of recovery, where it is possible to make an accurate assessment of their longer-term needs.
In March 2025, 83% of people (aged 65 plus) were able to return home from hospital with no formal support required (i.e., a package of homecare or a placement in a Care Home). 40.1% of people were able to return home following a period of time on a bedded pathway. Our ambition is for the proportion of people able to return home following a period of time on a bedded pathway to be as high as possible, evidencing the effectiveness of the reablement services provided by our intermediate care services.
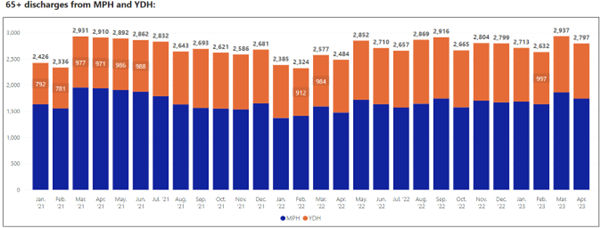
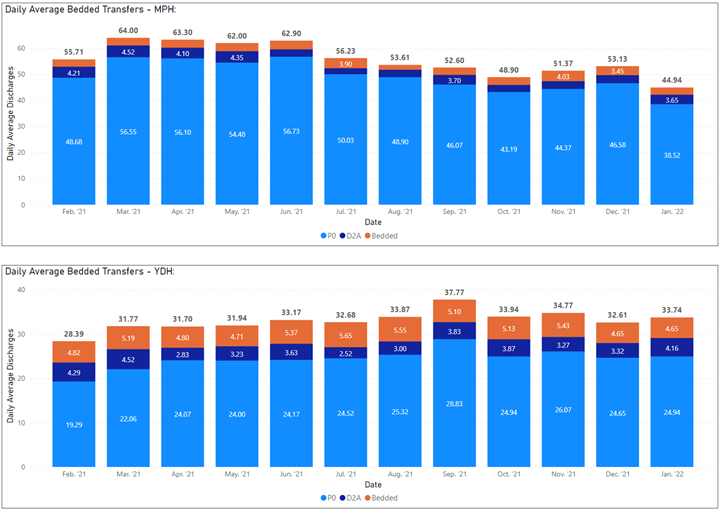
The charts below show the transfers from our main acute hospitals Musgrove Park in Taunton and Yeovil District Hospital.
On average our two largest acute Hospitals in Somerset discharge 2,760 people each month. Just over 13% of these people need additional support to reach their maximum potential and come to Intermediate Care for Reablement and assessment of their longer-term care needs.
Our Intermediate Care Services are made up of short term home based and bed based. Our Home support service is made up of a collaboration of up to 30 Health and Social Care specialists with 7 reablement home care providers who deliver over 3000 hours of support each week, along with 56 nights per week to help settle some of our more complex people to settle back home. Over 75% or people supported to go home with this short term help do not need longer term care.
The Community and Voluntary Sector are also a key partner in this provision and receive up to 360 referrals each month to help people with the information and support they need to stay connected and safe in their local communities.
Our top priorities for Intermediate care during 2025 are:
- Continue to increase flow in Pathway 1 (P1). We will:
- Continue to increase P1 starts with additional funding and modelling for long term performance.
- 24/25 increase starts 19%
- 25/26 increase starts by a further 40% by July 2025 (subject to initial funding)
- Improve average length of delay from Discharge Ready Date (DRD) to Discharge from an average of 4 to 2 days
- Ensure we consistently have the right P1 capacity in the right geography by developing flexible approaches and solutions to seasonal variation, rurality and acute escalation
- In turn we aim to decrease demand on Pathway 2 (P2) beds and de-escalate the Intermediate Care bedded provision
- Agree a P1 model for a provider led service to be recommissioned in 2026
- Manage P1 Length of Stay (LOS) to continue at a target 17 days and a 7 hour effectiveness target
- Improve acute P1 cancellations from a current average of 13 to 5 per week
- Increase P1 ability to support greater complexity by building in additional P1 capacity to support an average of 12% discharges.
- Integrate VCFSE with Move to Independence and low cost no cost community support solutions
- Reduce bedded demand via home first options and increase Pathway 0 to 85% (current average 83.8% July 24 – Jan 25)
- Consolidate bed modelling and further reduce demand by:
-
- Pathway 2
- Ensuring the right bed, in the right location, with the right support for P2
- Re-design the P2 bed pathways with a clear staffing model and bed resource that is dedicated to P2 rehabilitation.
- Phased bed de-escalation programme to support recommendations from the bed modelling.
- Pathway 3
- Disaggregating Pathway 3 from Pathway 2. Develop a spot purchased P3 model. The key aim is to support one move from acute to the right bed for complex people who are no longer able to stay at home, where they can have the support they need to settle and be assessed in a placement that will be able to continue to meet their long term needs.
- The model resource for Pathway 3 will support funding for 28 beds and a target LOS of 28 days.
- The Pathway 3 spot plan will commence in August 2025
- Pathway 2
- Improve and increase Voluntary, Community, Faith and Social Enterprise (VCFSE) involvement in Pathway 0 (P0) and long-term solutions for home first by reallocating VCFSE resource to acutes.
- Adopting the collaboration of community health and social care neighbourhood approach and align with Intermediate Care that support the new Neighbourhood health ambition for Better Care Fund:
- Population health management
- Modern general practice
- Standardising community health services
- Neighbourhood multi-disciplinary teams
- Integrated intermediate care with a ‘Home First’ approach
- Agree and implement key performance indicators to measure quality, performance and outcomes for users.